


Hospital leaders have to learn the behaviours needed to make sure change and improvements are embedded among staff
In this third lesson of a six-part series, I describe how leaders and leadership behaviours can enable a sustainable culture of continuous improvement.
Publishing one lesson a month, my goal is to share lessons from my evaluation of the five-year long NHS partnership with the US Virginia Mason Institute, and foster a global conversation about how to lead improvement within healthcare organisations and systems.
Each lesson will be followed by a ‘tweetchat’ on Twitter hosted by WBS in partnership with the #QIhour network. The lessons are summarised in Six key lessons from the NHS and Virginia Mason Institute partnership. You can join in the conversation via Twitter or LinkedIn using the hashtag #LeadingQI.
Panaceas for organisational change and improvement almost always highlight the requirement for leadership commitment from the top of the organisation.
Yet, leadership commitment is the most frequently cited barrier to successful implementation of improvement initiatives. London Business School professor Gary Hamel recently shared a tweet and accompanying graphic proclaiming: “Improvement fails because few leaders are capable of 1) imagining radically different future states; 2) approaching change systemically (vs looking for a silver bullet); and 3) persevering over the three to four years it takes to make deep change irreversible.”
While the sentiment resonates for many of us, I can’t help thinking there might be something amiss.
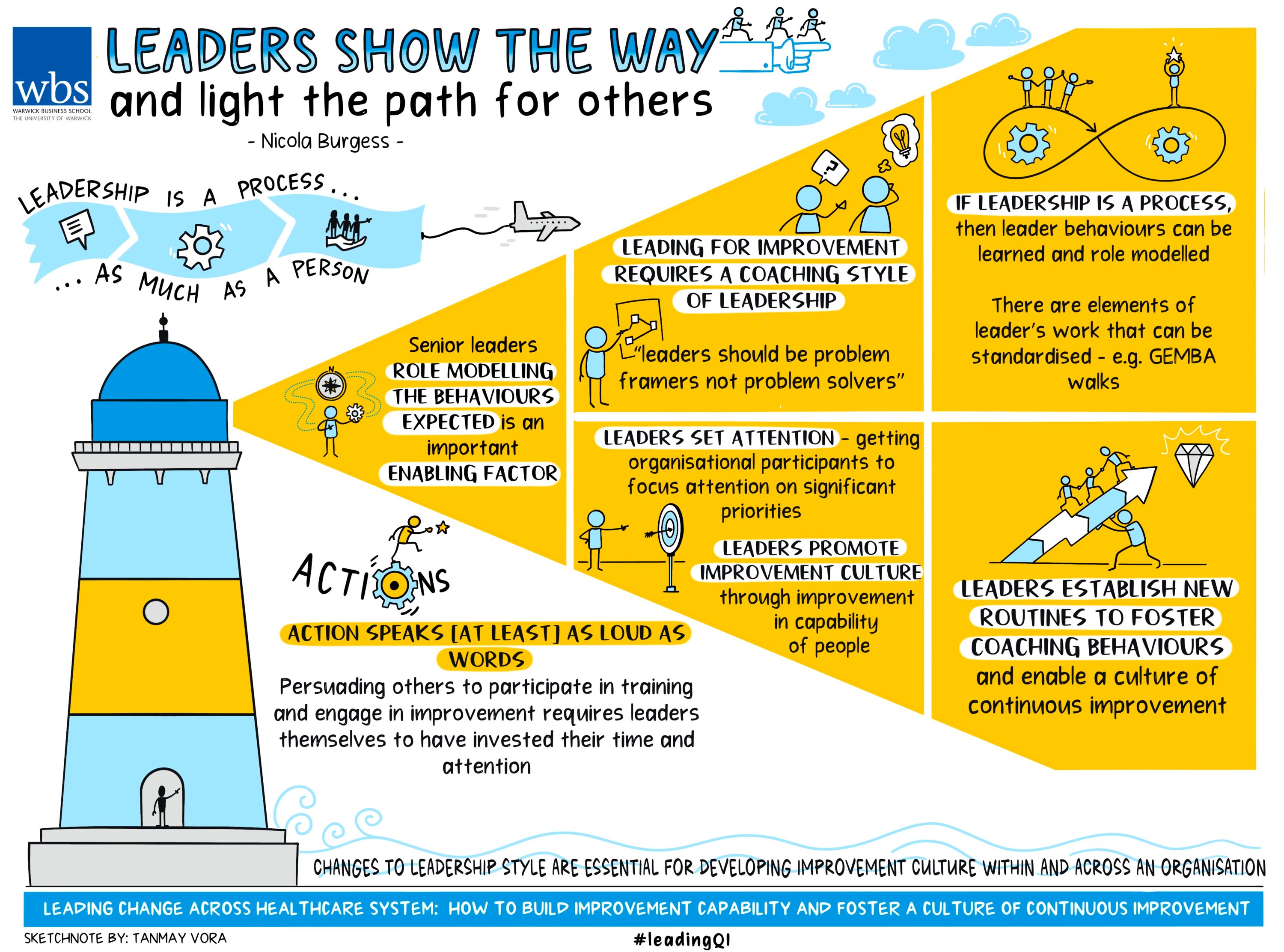
Leadership is a process as much as a person
When we talk about leaders failing to persevere with change initiatives, might we be guilty of blaming the person, rather than the process? The process being continuously shaped and constrained by conflicting demands and priorities of the wider system. In other words, blaming the person rarely yields a satisfactory solution.
But if leadership is a process, then leader behaviours can be learned, role-modelled, and even standardised (sort of). We’ll come back to that last point.
Learning leadership for improvement
The NHS partnership with the Virginia Mason Institute (VMI) involved five English hospital trusts adopting lean principles systematically via an improvement infrastructure, incorporating significant investments in leadership training and coaching.
This was evidenced at every level of the partnership and organisation: from the monthly meeting of the five hospital chief executives, where leaders learned from one another (see my blog for NHS Providers), to the rigorous training and certification of improvement specialists to form a centralised improvement team, who themselves were charged with training the organisation’s leaders in improvement methods.
Culture and leadership training
Initially, the Lean for Leaders training programme was targeted at more senior level leaders with the aim of moving gradually towards middle and then front-line leaders over time.
This tiered approach to teaching improvement methods played out differently across the five hospital trusts. An organisation’s ‘cultural readiness’ was directly correlated to the receptivity of senior leaders’ engagement with the training. To forewarn, the differences here were stark.
At one extreme, the organisation that appeared most ‘culturally ready’ for the improvement approach exhibited a palpable ‘excitement’ among senior leaders eager to learn about the methods and conduct their own projects.
At this NHS trust a waiting list was quickly established and maintained across the full five-year partnership. The training was quickly opened to all staff in leadership roles regardless of seniority or title.
At the other end of the spectrum, where organisational culture was less receptive to change, senior leaders were resistant to engage with the training.
Subsequently, a formal invitation was sent by the chief executive to ‘select’ individuals to request their participation. Some respondents expressed resentment of the training directive, some perceived it as punitive, and others were fearful about why they had been specifically chosen.
Very often these same respondents told us they benefited from participating in the course, applying the principles and methods in their own departments and encouraging others to learn and apply improvement methods.
Since the NHS-VMI partnership initially targeted senior leaders for training, some participants viewed it (and the corresponding improvement endeavour) to be ‘elitist’, fuelling animosity, suspicion, and creating an ‘us and them’ divide that was difficult to break down.
In sum, while organisational change almost always highlights the requirement for commitment from the top of the organisation, we need to recognise that leadership is distributed across the organisation vertically. It is also rendered more effective where it is diverse and inclusive.
The goal of a training programme such as the Lean for Leaders, is to achieve a critical mass, an ‘army’ of leadership actors engaged and championing the application of improvement principles and methods.
Why executive leaders need to do the training as well
Did the chief executives complete the Lean for Leaders training? Should they be expected to complete it?
The short answer is yes, they did complete it. But also no, not at the beginning, and not before other organisational members had made it clear that chief executive participation would be important.
The case for chief executives to complete mandatory training in lean improvement methods was not immediately apparent, but the importance of senior leaders role-modelling the behaviours expected of others emerged as an important enabling factor.
It was apparent through the evaluation that all chief executives had adopted new leadership behaviours as a consequence of their involvement in the partnership.
To illustrate, one frequently voiced leadership mantra that often made me smile was: ‘Leaders need big ears, big eyes, little mouth’; another was ‘leaders should be problem framers, not problem solvers’.
Both mantras remind us that improvement requires a coaching style of leadership, where a leader’s role is to listen, observe (by visiting the genba or the place where the work is done) and encourage employees to use improvement principles and tools to solve the problems they face.
Aligned to this is another popular mantra: ‘those who do the work know best how to improve the work’, and in case you haven’t had enough already there was also ‘better never stops!’
If we consider a leader’s role as one of ‘attention setting’ ie getting organisational participants to focus on priorities identified as significant, then leaders should be concerned with promoting a culture of improvement through increasing the capability of the organisation’s people, rather than applying tools of improvement themselves per se.
However, there was a growing plea from participants for the chief executives to complete the Lean for Leaders training. Subsequently, in 2019 the chief executives did participate in the training, learning the principles and methods of lean improvement alongside staff.
Actions speak [at least] as loud as words
Leadership theorist Richard Cyert asserts that a leader cannot succeed in persuading others to allocate attention in a desired direction without a strong intellectual position.
Hence, persuading others to direct their attention to participating in the Lean for leaders training and engaging with the improvement programme more generally requires leaders themselves to have invested their time and attention in the same.
It is a case of ‘actions speak [at least] as loud as words’; it’s also a demonstration of respectful behaviours that ultimately underpins a successful management system.
Ultimately, participation in the training by chief executives communicated to everyone that this is important. And few would argue they didn’t have the time if the chief executive did.
Leaders light the path for others
Senior leaders who ‘go first’ are sending a message that this is organisationally significant, and this is where staff must direct their attention.
That leader behaviours could be ‘standardised’ might seem a little extreme, but there are elements of leader work that can and should be. For example, the ‘gemba’ (also genba) walk discussed in lesson two is something that should form part of a leadership routine. Whether that routine is daily, weekly or monthly depends on the level of the leader.
Frontline leaders may benefit from daily genba walks, for example, while for senior leaders this might be a monthly activity. Developing leader ‘standard work’ can help establish new routines that foster coaching behaviours and enable a continuous improvement culture to grow.
In sum, changes to leadership style are essential for developing an improvement culture within and across an organisation. However, since health and care provider organisations exist within a wider system of governance and oversight, the efficacy of a coaching style is enhanced when similar coaching behaviors are adopted by leaders across all levels of the system.
The third tweetchat on leaders lighting the path for others will be held on Tuesday March 28, 7-9pm GMT. Follow the hashtags #LeadingQI and #QIhour to join in and learn more from the NHS-VMI Partnership.
Nicola Burgess is Reader of Operations Management and teaches Operational Management on the Distance Learning MBA plus Digital Innovation in the Healthcare Industry on the Executive MBA.
Follow Nicola Burgess on Twitter @DrNicolaBurgess.
More lessons from the Virginia Mason Institute – NHS Partnership:
1 Build cultural readiness as the foundation for better QI outcomes
2 Embed QI routines and practices into everyday practice
3 Leaders show the way and light the path for others
4 Relationships aren’t a priority, they’re a prerequisite
5 Holding each other to account for behaviours, not just outcomes
6 The rule of the golden thread: not all improvement matters in the same way
For more articles on Healthcare and Wellbeing sign up to Core Insights here.
 X
X Facebook
Facebook LinkedIn
LinkedIn YouTube
YouTube Instagram
Instagram Tiktok
Tiktok